
Ebola.
Why is the outbreak different this time?


Ebola has returned to Africa and this time, the World Health Organization declared it a Public Health Emergency of International Concern (PHEIC) on May 17, 2026. In the last notable outbreak of 2013-14, it was not declared a PHEIC for almost a year, when many of the same factors existed that would make it one. I will share the algorithm for determining whether you have a PHEIC under the International Health Regulations and discuss how this happened.
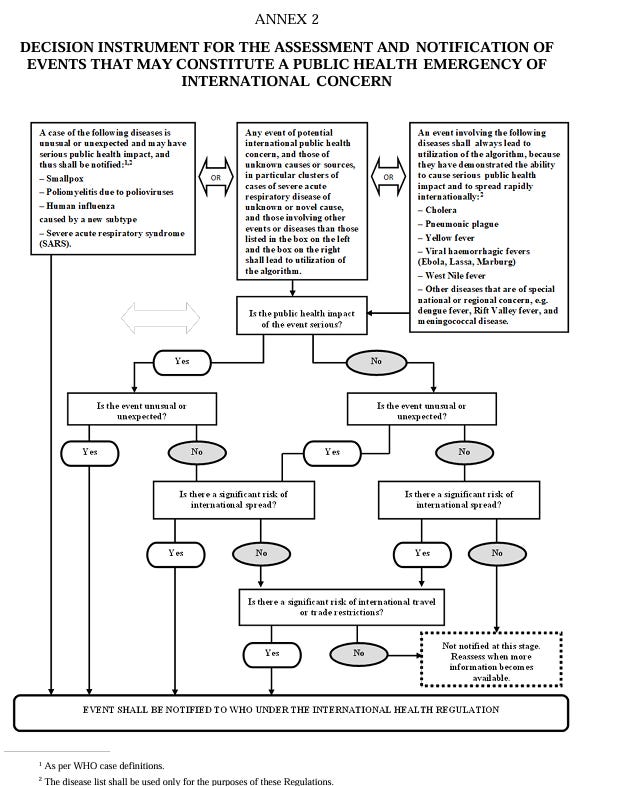
This algorithm is typically used to determine when a member Nation should notify WHO of any outbreak or case. These factors are also considered when WHO considers whether a PHEIC should be declared. The Director General in his remarks on May 19, 2026 said this, “This is the first time a Director-General has declared a PHEIC before convening an Emergency Committee. I did not do this lightly.” 1
The Director-General appointed an Emergency Committee on May 20, 2026.
The mechanism to declare a PHEIC was created in the International Health Regulations that became final in 2005. This regulation had been in development for some years, but there is no doubt that the 2003 SARS outbreak in China (when China failed to report the novel respiratory virus) gave momentum to completing the binding regulations. Since that time, nine official PHEIC declarations have been made, three of them for an Ebola outbreak in Africa:
2009-2010, H1N1 (”Swine Flu”) Influenza Pandemic
2014 - present, Poliomyelitis
2014-2016, Western Africa Ebola Epidemic
2016, Zika Virus Epidemic
2019-2020, Kivu Ebola Epidemic (Democratic Republic of the Congo)
2022-2023, COVID-19 Pandemic
2022-2023, Mpox (Monkeypox) Epidemic (Clade II)
2024-2025, Mpox Epidemic (Clade I)
2026-Present, Ebola Epidemic [Ituri Province (Congo) & Uganda]
So what was different about this outbreak? First there was a lot of criticism for the slow response from the West to the outbreak in 2013. The problem is always framed as “what is the risk to Europe?” rather than what can we do to help contain the people in Africa. This political cartoon captured that public perception:
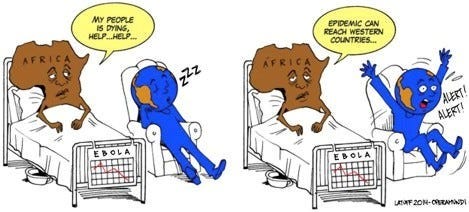
From, Adnan I Qureshi, “West Saharan Response to Ebola Virus Disease Epidemic,” chapter in Ebola Virus Disease: From Origins to Outbreak (Elsevier, 2016).2
The Director General’s rush to declare a PHEIC even before the committee was convened showed this urgency he felt existed but he also could have felt pressure from the past foot-dragging.
The stated reason was for all of the factors in the PHEIC algorithm. Naming this as factor number five, the Director General stated that the Bundibugyo virus (the rarer strain of the three strains of Ebola), unlike the other two Ebola-Zaire strains, does not have a known vaccine or therapeutic.3 (However, during the 2013 outbreak, there was no known vaccine; however there was an experimental one, discussed below, approved for experimental use only after the PHEIC declaration. In addition, there was a different Director General, Dr. Margaret Chan.4)
The slow response in 2013
I wrote in Feb 2025 about the slow response of the West to the Ebola epidemic in Western Africa in 2013. A PHEIC was not declared until 2014. There was another outbreak in the DRC (Congo) in 2018-2019, that was complex and difficult and for that, another PHEIC was declared.5 Since that time there have been minor outbreaks, but not until this week, has any of these risen to the third PHEIC declaration.
The first vaccine used for Ebola was in 2014 in Western Africa during an epidemic, there. I will excerpt that article here (you can read the entire article here at this footnote).6
Growing Vaccines in Plants—ZMapp
ZMapp is a therapeutic that was developed as a rapid response to Ebola in the 2013-2014 epidemic. The World Health Organization and the western hemisphere was slow to respond to the epidemic emerging in three of the countries of western Africa (Ivory Coast, Guinea, Liberia). But once Ebola began to spread beyond Africa, the efforts to develop a vaccine and therapeutics accelerated their development. Exacerbating the situation, there was an intense distrust among the people of west Africa of western countries profiting from a vaccine as well as a distrust of their own corrupt governments.
Meanwhile, over the course of years, hundreds of U.S. scientists had been engaged in research for a vaccine or “cure” for Ebola.
The reproduction of cells in the tobacco leaf had been an ongoing research process already for about a decade. When the opportunity arose to apply this urgent need to develop antibodies to Ebola, the company, ZMapp was successful with this biotechnology process. A company in Kentucky was hired for the growing process, Kentucky Bioprocessing, a subsidiary of Reynolds America, experts in tobacco cultivation.
Although ZMapp had not been tried on any human subjects, it was determined to meet the experimental use category (EUA) of FDA for use on Ebola patients in October 2014. The World Health Organization also determined it met the requirements through its emergency use in public health emergencies protocol, Monitored Emergency Use of Unregistered and Investigational Interventions (MEURI). 7
A brief account of the course of the Ebola epidemic in west Africa is given in a book by Michael B.A. Oldstone and Madeleine Rose Oldstone, in Ebola’s Curse, 2017:
At this Doctors Without Borders center where Khan now awaited help were others infected with Ebola and also gravely sick. Yet, the center had barely enough ZMapp for three or four persons. Despite his eminence, Dr. Khan was not told that ZMapp was available. The choice of which patients received ZMapp lay primarily in the hands of a team at the Canadian company that made ZMapp and members of Doctors Without Borders at the Kailahun treatment center. But they were not the only decision makers. Also involved were representatives from the World Health Organization, Center for Disease Control and Prevention, and National Institutes of Health. Despite the danger of progressive disease as time passed, the health officials deliberated while considering that neither the antibody’s therapeutic effectiveness nor its side effects were known. In the end, they decided not to tell Khan about ZMapp or ask if it could be used on him. Instead, the ZMapp was transported to Guinea where two Ebola-infected victims were treated: a volunteer American physician, Kent Brantly, and a volunteer American health worker, Nancy Writebol, both from Samaritan’s Purse charity. Later a priest, Miguel Pajares, from Spain was also given ZMapp. The first two survived but the priest died.
The WHO approved ZMapp in the 2018-19 Kivu Ebola outbreak in the Democratic Republic of the Congo under the MEURI protocol. However, the newer drug, REGENERON, was purportedly more effective than ZMapp and in August 2019, the Democratic Republic of the Congo’s national health authorities, the World Health Organization, and the National Institutes of Health announced ZMapp would no longer be used to treat Ebola because REGENERON was said to be much more effective. REGENERON was developed in response to the COVID-19 need for therapeutics, was the first drug to be approved by the FDA as an approved treatment for Ebola, October 2020.
Final thoughts
The urgency with declaring the Ebola outbreak in DRC and Uganda by the Director General before a committee could even be appointed, seems to have turned on the one key different from the previous outbreaks — because it is the rarer strain of Ebola, which has no vaccine or therapeutic.
But when the rest of the world asks if they should be concerned about Ebola reaching them, the answer may be “yes” or a PHEIC may never be declared and Africa might never get the help they need.
_________________________________________________________________________
May 25, 2022 I wrote the first unintended consequences article, and wrote one each week from then on. I had about 25 subscribers and about 41 views on my first article. Thanks to all of you I have about 500 subscribers and as many as 5,000 views every week. This marks the four year anniversary and thank you for going on this journey with me.
https://www.who.int/news-room/speeches/item/who-director-general-s-opening-remarks-at-the-emergency-committee-on-ebola-epidemic-in-the-democratic-republic-of-the-congo-and-uganda---19-may-2026
https://www.sciencedirect.com/book/9780128042304/ebola-virus-disease (open source at Science Direct).
https://web.archive.org/web/20260520044450/https://www.who.int/news/item/17-05-2026-epidemic-of-ebola-disease-in-the-democratic-republic-of-the-congo-and-uganda-determined-a-public-health-emergency-of-international-concern
https://en.wikipedia.org/wiki/Margaret_Chan
https://www.who.int/europe/news-room/fact-sheets/item/ebola-outbreaks